 |
|||||||||||||
|
|
|||||||||||||
|
Diabetes prevention through genetic testing and lifestyle management
Introduction
What if I told you that I could get information that could potentially save your life or, possibly, make it a lot better? This is the possibility of genetic testing. Of the many genes identified, genes play a complicated but predictable role in whether or not we develop diseases. Some of these relationships have been identified, others only hint at possible interactions. We must take responsibility for our own health by utilizing the best tool we have: our own bodies. Despite the fact that disease plagues us, our bodies are smart. They learn, they adapt to extremes and they are the result of 5 to 6 million years of evolution (Stringer 1994). Who is going to argue with that kind of trial and error? How do we go about this? Education and acquisition of knowledge. The field of biology is still in its infancy of answering all questions science aims to answer and thus "scientific proof" is never 100%. We can work with what we do know about the human body and its internal and unseen processes and use these to our advantage. Currently there are over 1,000 genetic tests available that are disease specific. How can we use this to prevent disease?
There is no question about the high cost of disease which afflicts our nation. This cost is not only monetary, but also costs our communities and families as well. As the field of genetics-based pathology progresses, we are able to recognize many susceptibilities to disease that lie within our own genetic make-up. We still have a long way to go to decipher all of the intricacies of how environment interacts with our genes. This is often the topic of genetics based psychology, pathobiology and of course, genetics, among many others. Until the time comes where we can piece together all of these very complex systems, we only have correlational information available to us. Correlation is not causation as any scientist will tell you. However, correlation coefficients are used to predict one variable in terms of another. A positive correlation between two variables shows that there is a high chance that the two will occur together, although, not necessarily simultaneously. A 100% positive correlation is the strongest correlation, but of course most correlations fall somewhere below that (figure 1). A strong positive correlation is the basis for my idea. This idea, aims to use the information gathered from empirical evidence which shows strong correlations for genetic variation and how variation influences the onset of different pathologies.
So much of western medicine is concerned with "industrial" demand which is mostly post-onset treatment. This framework (while is the only option in some cases) is misguided. Despite the current view of treating symptoms rather than underlying problems, more people are realizing the benefits of leading healthy lifestyles. There is a way we can take this a step further, and that is through increased knowledge, guidance and education.
Background
During my time in the Department of Pathology doing research, our team set out to develop a test which detected allele variance in the promoter region of the gene which encodes SLC6A4, the serotonin transporter protein (figure 2). We planned to use standard molecular biology methods of polymerase chain reaction paired with gel electrophoresis and sequencing. A correlation between a variant referred to as the "short" form (located in the non-coding region of the gene's promoter) to development of Post-traumatic stress disorder was established by previous investigators. This short form constitutes a 44 bp difference in length when compared with the long version of the allele. There are other variants as well which have been identified in the SERT gene. There is the long form with the single nucleotide polymorphism (G) which is believed to be expressed much like the short form. It is commonly referred to as the low expressing (L) allele.
I desired to see if we could use something other than PCR to detect variation which might make testing more available to the general public in the future. My first problem was getting the DNA, which I planned to use buccal swabs (a standard for acquiring DNA) to extract DNA. Initially, I turned to thinking about detection by melting point, looking specifically at single nucleotide polymorphisms (SNPs) which would allow for detection of the variant by heating. I then consulted Maggie Werner-Washburne and Paul Szauter who suggested fluorescent tagged oligonucleotides and also ligation sequencing. I then thought of trying to come up with a way to combine a blotting technique somehow with paper chromatography like in chemistry. Paper chromatography, as used in the fields of chemistry as well as molecular biology is useful for quick visualization to detect the presence of a molecule/compound using reactive dyes that simply use nitrocellulose paper along with chemical tagging to produce a visual reaction (Zhang et al. 2000, Rule et al. 1996) I aimed to do this using a fluorescent probe as suggested that could hybridize to the region of interest located in the long version of the allele. Plus an additional probe that would hybridize to the sequences through where the deletion on the short version would appear, but since that region would be missing it will go directly from the end of the short version onto the neighboring sequence surrounding the region. The questions I aimed to answer during this process were:
1. Is there a way to develop the probe so that it can hybridize quickly and consistently?
a. Southern blotting by way of random-oligo-primed-synthesis is a widespread method used to probe for specific sequences. This is typically used in conjunction with Polymerase Chain Reaction using expensive enzymes. Is there a way to bypass this part of the process? Can we utilize other ideas in molecular biology to solve this problem?
b. Often, people use immunohistochemistry to detect the presence of certain compounds expressed in the cell. This is the case in Western Blotting but often we are detecting using antibodies
2. Can a similar approach be used for our purpose?
Right around this time, Mr. Szauter suggested that I redirect my project because genome-wide sequencing was becoming highly available and very inexpensive. He suggested that any test I could create would be obsolete in the next 5 to 7 years. At first, this seemed to be a roadblock.
This approach also presenting other problems such as getting false negatives in my detection results.
Then I thought:
3. How can we use this gene variation information?
a. Taking PTSD for instance, having knowledge that you are at risk of developing this potentially disabling disease
4. Would it be useful to know your genotype?
5. If genetic testing is becoming more widely available, how often are people getting tested?
6. What are they typically tested for?
7. Do they know how to interpret their results?
8. What other genetic correlations are available that could help in the prevention of the disease?
This inspired a quest for investigation into the genetic basis of pathology. I decided to keep PTSD and the information I had to identify variants of SLC6A4. After all, the research shows a 30% increase in vulnerability to develop PTSD when exposed to trauma and also having the short form of the allele (Heils 1996). I have included a cost based analysis of PTSD based on its prevalence amongst war veterans (figures 3,4,5) (figure 8).
Based on this information, I intended to ask Veteran's Affairs to conduct genetic testing on new recruits. This issue raises some ethical concerns about how this test can be used.
There is a law against discrimination based on genotype, and surely this should not be used as a discriminatory factor.
It should be used as a way to circumvent the onset of the disease. This is especially important because of the sheer lack of knowledge in its' etiology and the lack of effective treatment of the disease.
As in medicine, the field of psychology is often lost as to how to effectively treat disorders-especially in the long term. Often, sedatives are used for a variety of issues which don't serve to actually change the underlying causes of disturbance. Other treatments are addictive and some just simply aren't effective after some time. This is ultimately due to lack our lack of knowledge in the psychological community and its corresponding medical counterpart, Psychiatry. This limitation is potentially dangerous to the consumers of such medications and brings forth the importance of lifestyle maintenance and the need for education in disease prevention.
Genes which influence the development of pathologies are often revealed through twin studies. Monozygotic twins serve as great models to explore when one twin develops a disorder another does not. In PTSD, twin studies have been used to calculate the heritability of the disorder (Koenan 2007). Studies show that the heritability of PTSD is about 30% (Koenan 2007). The test I have been working on could help prevent the onset of PTSD one day. I thought this was a great place to start, essentially it is preventative medicine. My test is ultimately geared towards the military and so I thought that maybe the military would be interested in other genes and psychological problems. I came up with a list of psychology-related problems that could have genetic influence based on my previous studies in the Department of Psychology.
1. Depression
2. Anxiety
3. Drug/Alcoholism
4. Anti-social personality
These were the four major topics I decided to research. Research shows that depression, anxiety and possibly alcoholism and drug addiction all show strong heritability (Goldman 2005).
Would the military be interested in this? Possibly. However, I felt that if they were to test new recruits for these types of susceptibilities, this could eventually lead to discrimination, despite the current legislation against it. I felt it would be appropriate to abandon my efforts based on my personal ethics. I felt that people should have the right to access this type of information if they so desire, but I had to return to my main focus: How can we use this information to help people by improving or even saving their lives?
Genetics and pathology, along with new trends in nutrition (like eating organic and avoiding high fructose corn syrup) gave me an idea. What disorders and diseases (psychological or other) may be influenced by genetics? I decided to start research online for genetic tests which are currently available. I came across a long list of tests currently used. These included Tay Sach's, Huntington's diseases and various others such as sickle cell anemia. Most of these genetic tests are gotten through referrals by a clinician. Many of these tests are specific amongst certain racial populations. Some genetic variations between humans of different races have been shown to be evolutionarily advantageous (Miller 2012).
Paul Szauter sequenced his genome through the web site 23 and me. They mail a "kit" which includes information on how to get a buccal swab from your cheek. You mail the kit back and they sequence your genome. It includes "fun" things that you can find out about your genome like what percent Neanderthal you are, if any.
Paul also disclosed to me that he was heterozygous for the SLC6A4 short and long allele. In fact, most European and European Americans are heterozygous for the short and long allele. Paul also discovered that he also carried an allele that left him vulnerable to developing hemochromatosis. A devastating disorder which is not often diagnosed until extensive organ damage has already occurred. In this disease, excess iron uptake is occurring in the body's tissues. Currently, a test for this type of disorder is not widely available. This turn of events led me to ask again what else we might be able to find out about our susceptibilities through genetic testing.
I feel that there is a need for testing to be widely used, but I also recognized the need for genetic counseling thereafter. I thought that maybe I could design a curriculum to help people understand what genotypes mean and how to understand their genome and any genetic testing they would go through. I spoke with Paul on this, and he directed me to the "23andme" site where they had videos about genes, genotype and how genes interact with environment. It was titled "genetics 101." They did a fair job of explaining things at an appropriate level. Seeing that at least 23andme were off on a good track to developing something, I shifted my focus back to genes and their link to the development of disorders.
"Perhaps we could attack the biggest things first, and go from there?" I thought to myself. What are the biggest problems in disease facing Americans? I then decided to look into which diseases claim the most lives in our country. On that list:
1. Heart Disease, 599,413
2. Cancer, 567,628
3. Chronic Lower Respiratory diseases, 137,353
4. Stroke, 128,842
5. Accidents 118,021
6. Alzheimers 79, 003
7. Diabetes, 68, 705
8. Flu, Nephritis, suicide <68k
The United States Center for Disease Control collects ongoing statistical information on the types of diseases which are most common in our country and are also the "biggest killers." If you notice, Diabetes only accounts for ~4% of deaths per year of the biggest killers (figure 7). In contrast to this seemingly small number, the cost of diabetes to the healthcare industry vastly outnumbers some of the other diseases which cause death. This is reasonable because diabetes requires a lot of medical maintenance (figure 9). I immediately wondered:
1. "does diabetes have a genetic component?"
2. How can we as a society prevent diabetes?
3. How does health condition influence diabetes development?
There are two main types of Diabetes type 1 and type 2. Type 1, people are born with or the onset is in early childhood and type 2, which people develop later in life. Type 2 is often referred to as "adult-onset" diabetes. Type 2 diabetes accounts for about 90% to 95% of diagnosed cases (CDC 2012). Type 2 is first diagnosed as "pre-diabetes" in which people show higher than normal blood glucose levels. By this time, many clinicians believe that damage to the cardiac and nervous systems is already occurring (CDC 2012). Several studies have shown that overweight pre-diabetics who have certain TCF7L2 variants have a 55-70% chance to develop Type 2 diabetes within 3 to 5 years after their initial diagnosis (NIH 2012). Research shows that the heritability of type 2 diabetes from one gene single nucleotide variant in TCF7L2 is 26% (NIH 2012). This refers to the fact that a variance in the gene TCF7L2 contributes 26% to the development of diabetes (CDC 2012). 74% are other factors (other genes or environmental) that contribute to the development of diabetes. What heritability measures is the amount of diabetes development which can be attributed to the presence of this particular variant. It does not demonstrate a cause-effect relationship nor does it take into account other genes which may contribute to the development of diabetes. One article cites that multiple copies of this variant in the genome doubles your chance of developing diabetes (EurekAlert 2012). The gene variants of TCF7L2 are single nucleotide polymorphisms, rs12255372 and rs7903146. 11 genes have been identified which contribute to diabetes development. These genes include PPARG, FTO, KCNJ11, NOTCH2, WFS1, CDKAL1, IGF2BP2, SLC30A8, JAZF1, and HHEX. The heritability of all of these genes has yet to be determined.
The lifetime risk for males to develop diabetes is 1 in 2, and 2 in 5 for females. Since all people who develop diabetes are of unknown genotype, further study is needed to assess how much genotype actually influences the development of diabetes. It is reasonable to assess that there are multiple contributing factors, but since the lifetime risk is so high, the exact quantitative evaluation of these factors is unknown but obvious.
If 76% of associated risks to develop diabetes stem from other causes, what are those causes? For some time, it has been common knowledge that being overweight has a positive correlation with diabetes development. What is it about people who are not overweight that leads to prevention? Maintaining your health is a theme that comes up all the time. How can we help people do this? The Diabetes Prevention Program (DPP) research showed that lifestyle intervention reduced the development of type 2 diabetes by 58% (NIH 2012). This type of intervention, does demonstrate a cause-effect relationship. How was this measured? The information was obtained by recent study conducted by the National Institute of Health in which participants were monitored through a prevention program which included coached lifestyle management.
The cost of lifestyle intervention is ~$4,601 cost per year versus ~$13,000k per year treating a diabetic (NIH 2012). The difference here is obvious but also very encouraging. Also, throughout the study, the quality of life as measured by mobility, level of pain, emotional outlook and other indicators was consistently better for the lifestyle group (NIH 2012). Who'd have thought that taking care of your body would be so positively correlated to overall health? I think most people want to take care of their bodies but they don't necessarily know how. This is where the healthcare community can come into play.
Diabetes is highly preventable. We need to test before the pre-diabetes phase as part of a routine physical exam and combine this with coached lifestyle management. We can expect to see an even sharper decrease in development. Genetic testing is available but is typically around 1k for a complete screen. Genes: TCF7L2, PPARG, FTO, KCNJ11, NOTCH2, WFS1, CDKAL1, IGF2BP2, SLC30A8, JAZF1, and HHEX. This is outrageously expensive and simply out of reach for people who are at the highest risk for developing diabetes like people of low socioeconomic status and minority populations. However, there is a demonstrated need to increase the availability of genetic testing and decrease the cost based on the high numbers of diabetes cases afflicting minority and low SES Americans. The existing Diabetes Prevention Program (DPP) lifestyle intervention method includes the following:
Early intervention could save us over $390,000 per person over his or her lifetime.
While the variance in TCF7L2 may increase your susceptibility to develop the disorder, it is environmental interaction with the genome which directly influences whether or not you actually develop it. The reduction of development was even greater, 71%, among adults who are 60 years or older (NIH 2012). This clearly shows that gene-environment interaction is extremely important in the development of the disease. In psychology, this is commonly known as the nature versus nurture debate. This complex etiology is a perfect example of this theory and also can be applied here. We should use both genetic testing and lifestyle management in combination to decrease the numbers of cases that emerge. Prevention or delay of type 2 diabetes with lifestyle intervention has been shown to persist for at least 10 years through current research (CDC 2012). While there is a medication to suppress the on-set of diabetes, research shows lifestyle interventions are more cost-effective than medications (American Diabetes Association 2012).
Wouldn't it be better for our healthcare providers to be more active in providing preventative care rather than just dolling out pills? Since all of the effects of medications are generally unknown, we should opt for lifestyle management anyway. We know that leading a healthy lifestyle provides the maximum output for overall health, not just diabetes.
How can I make genetic testing easier and more widely available? How can we make improvements to the existing diabetes prevention plan?
The current cost of a PCR reaction is $15-25 in PCR reagents per test (NEB 2012). Sequencing of the DNA collected post-PCR reaction typically costs $8-12, depending on the method you use to prepare the DNA for sequencing (Davis Sequencing 2012). A DNA isolation kit costs $2/per sample (Qiagen 2012). Depending on the method you use to extract and collect DNA, the cost varies. The Oragene kit is $16.37 per sample (DNA Genotek 2012). Custom primers for the PCR reaction vary in cost but they are not typically expensive. The point here is that it would likely cost <$100 dollars per test to genotype people for variants of TCF7L2. How can we reduce the cost of this test?
1. Somehow try to design a cheaper test
a. Can we just design something that will detect a particular set of two or more SNPs, in bulk to save on cost?
b. Use something other than PCR?
Upon further research into this topic, I discovered Sequenom technology core. They conduct genotyping at the cost of .19 cents per sample submission. This is still after the PCR reaction has been carried out (Human Genetics Division Genotyping Core 2012). This makes the cost and preparation a little cheaper. After discussing this with Paul, he assured me that the price of genotyping would be likely to drop in the next few years and that making a new test would not be useful because it would become obsolete. After taking this into consideration, I shifted my focus, entirely, to the next problem: making the test and prevention program widely available.
2. Try to persuade insurance companies to cover the cost of genetic testing and the prevention program
a. This seems like a reasonable approach because of the cost-effective outcome of utilizing genetic testing and lifestyle management compared to the cost of treating people with diabetes
After a brief discussion with Paul about this issue, he advised that I steer clear of insurance companies. This is because he feels that they are out to take advantage of people. While I understand his perspective, I feel that they are in a perfect position to implement changes because they are interested in saving money. Afterall, they are the ones who end up having to pay a large portion of the medical costs of patients who are being treated. They are also in a position to want to save funding, because they are a business. The cost of the prevention program ~$4,000 plus the current cost of genotyping still falls far below the cost of treating someone with Diabetes type II. As far as the medical industry itself, since it is an "industry" they may be less inclined to keep people healthy unless under pressure by insurance companies to decrease costs. Who else is in a position to make changes? The U.S. government.
Every year, leading health professionals meet with government administrators (including President Obama) to form and discuss new policies regarding healthcare. This is a cabinet dedicated to the goal of keeping Americans healthy. Their official title is the U.S. Department of Health and Human Services. They aim to increase healthcare quality and decrease costs. They are also in a good position to implement changes regarding health policy, if they can get votes in the legislature. However, pleading my case at this governmental level will expose the idea so that others could take an interest in approaching this problem.
Proposal
1. Increase the availability and use of genetic testing by educating healthcare providers in multiple fields and specialties about how to extend the opportunity to their patients. Help health care providers learn to identify at-risk patients, how to speak about the benefits of the DPP program, how to enroll their patients and how to speak about gene-environment interactions at an appropriate level. Employ health insurance companies to cover the cost of genetic testing to identify those at higher risk.
2. Increase the availability of DPP through government funding, or ask insurance companies to fund it through health plans.
3. The diabetes prevention program currently has a lot of great aspects. It includes personal one-on-one management assistance and supervised physical activity sessions. One thing I would add is for insurance companies to offer incentives and discounts for showing proof of physical activity participation. Also, for those who can demonstrate that they are able to keep up their activity levels on their own, they should have status check-ins rather than just supervised physical activity. They should still have all the visits and the 16 week course requirements.
If we are serious as a nation about fighting diabetes and potentially saving trillions of dollars over time, we need reform. In the scope of the problems facing our nation as to the cost of healthcare, these changes are not that large. The possible impact on our communities is priceless. It would be comparable to trying to put a price on happiness or life itself. We have such incredibly knowledgeable and intelligent people who have a lot to contribute in our healthcare system and the sciences. We must work together to improve our nation's health. To make a difference for our own future and the future of our country, guide and encourage Americans to take personal responsibility for their health. To send a clear message to Americans about the importance of lifestyle management, it must come from people they trust. At a time when our country's financial situation is uncertain, it is also important that we find ways to decrease spending. These changes will require setup costs, but will save us a lot in the long term and should not be considered to be a risky venture. Our health is worth investing in on a a personal and societal level.
In conclusion, my project started out on a very different path than I intended but I am excited about the progress I have made on a personal level to expose what is most important to me-improving the lives of others. This fulfills a deeply personal goal of mine which has been instilled in me from the time I was a child. I am a native New Mexican, who comes from a background of the practice of traditional medicine. This has influenced the way I view medicine substantially, although I didn't recognize the benefits of it until my adulthood. An outline of the personal path I have taken through this project is viewable in figure 10. This project helped me to dig within myself and truly follow what I believe is important.
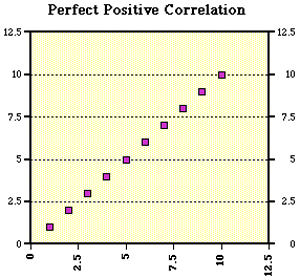
Figure 1. Shows a perfect positive correlation between. The X axis would be the presence of variable a, and according to this model you can predict the presence of a second variable according to a mathematical model. If an increase in one variable tends to be associated with an increase in the other then this is known as a positive correlation.
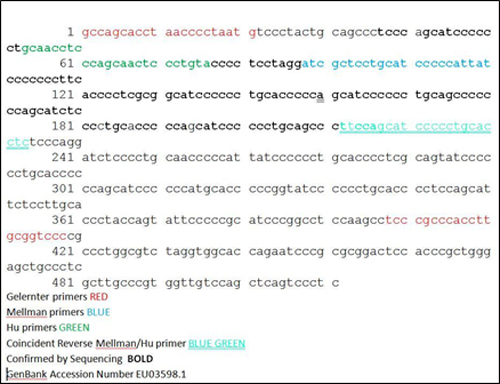
Figure 2. Shows the sequence of SLC6A4(long form) with the design I used to identify the allele using nested primers with polymerase chain reaction and gel electrophoresis and sequencing.
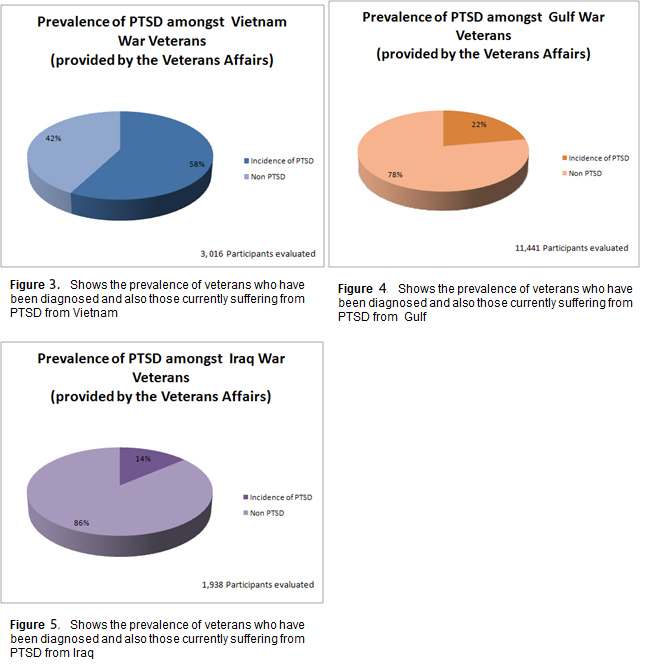
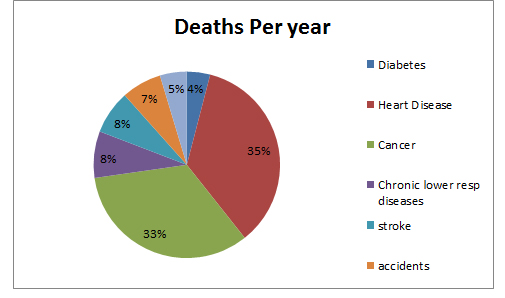
Figure 7. Shows the percentage of deaths per year in the United States by the top killing diseases.
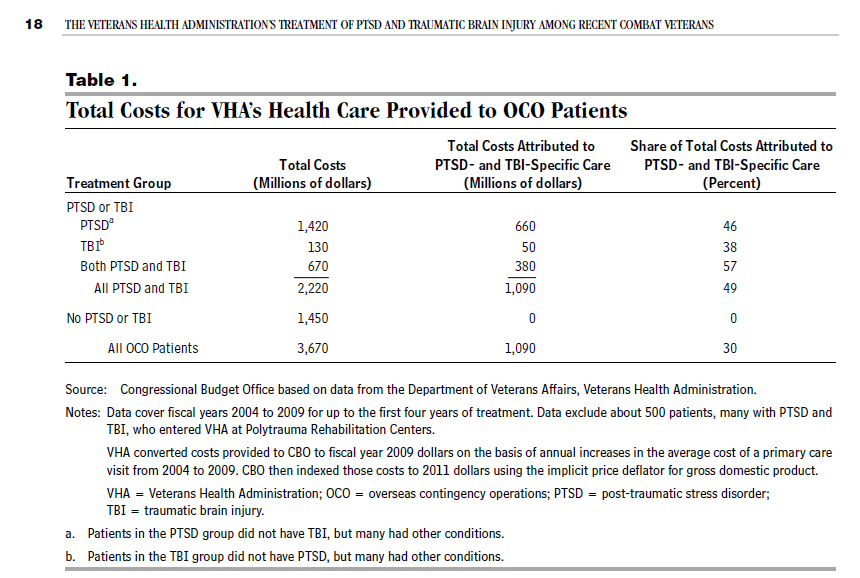
Figure 8. shows the cost of PTSD to the veteran's affairs, 1.4 milion is the total cost of PTSD in a five year period of 2004-2009
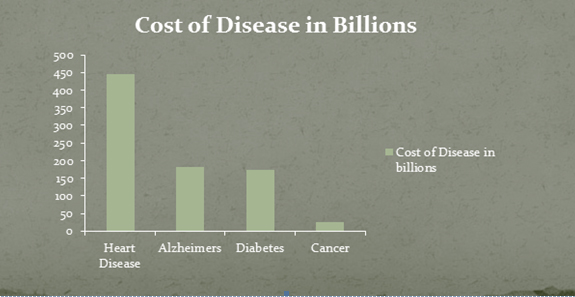
Figure 9. The cost of maintaining treatment of people with diabetes in the United States. Data from the year 2007.
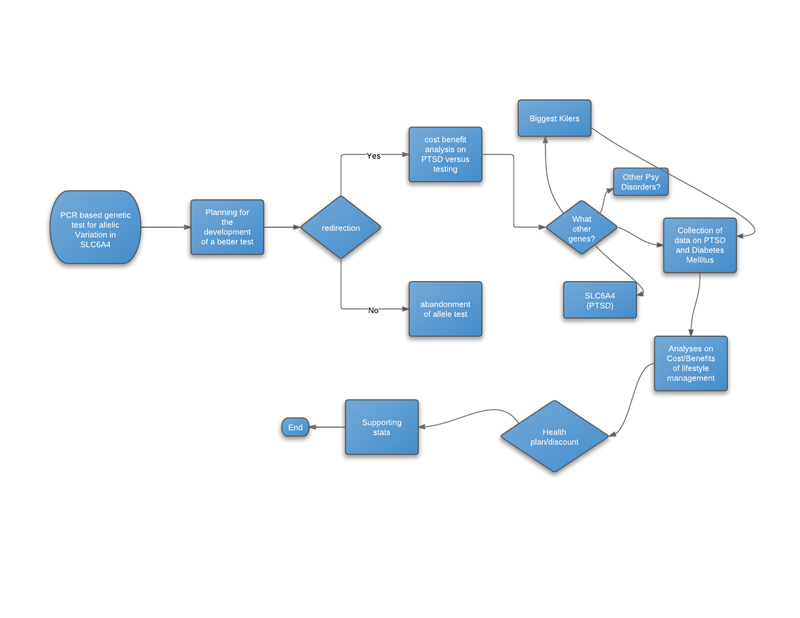
Figure 10. Project Progress, went from genetic testing for PTSD genes to using genetic testing in combination with lifestyle management as a plan to fight diabetes and persuade lawmakers and insurance companies to implement the changes
References:
"Congressional Budget Office." (CBO). Web..
"Diabetes Gene Carries Similar Risk to Obesity." Diabetes Gene Carries Similar Risk to Obesity. EurekAlert. Web. "Epidemiology of PTSD." Epidemiology of PTSD. Veteran's Affairs. Web. The role of genes in defining a molecular biology of PTSD. R Yehuda et al. 2011
"Gene Testing." Gene Testing. Web. "Genetic Testing Registry." National Center for Biotechnology Information. U.S. National Library of Medicine. Web. "NIH Study Finds Interventions to Prevent Type 2 Diabetes Give Good Return on Investment, March 22, 2012 News Release - National Institutes of Health (NIH)." U.S National Library of Medicine. U.S. National Library of Medicine. Web. "Sequenom Technology Core." Sequenom Technology Core. Http://hg.wustl.edu/info/Sequenom_description.html. Web. "Taq DNA Polymerase with Standard Taq Buffer (M0273), Routine PCR, NEB." Taq DNA Polymerase with Standard Taq Buffer (M0273), Routine PCR, NEB. Web. Primary sources
Bearer, E. L., Zhang, X., Janvelyan, D., Boulat, B., & Jacobs, R. E. (2009). Reward circuitry is perturbed in the absence of the serotonin transporter. NeuroImage, 46(4), 1091-104. Elsevier Inc. doi:10.1016/j.neuroimage.2009.03.026
Grabe, H. J., Spitzer, C., Schwahn, C., Ph, D., Barnow, S., Ph, D., Lucht, M., et al. (2009). Polymorphisms and the Susceptibility to Posttraumatic Stress Disorder in the General Population. Psychiatry: Interpersonal and Biological Processes, (August), 926-933.
Gelernter, J., Kranzler, H., & Cubells, J. F. (1997). Serotonin transporter protein (SLC6A4) allele and haplotype frequencies and linkage disequilibria in African- and European-American and Japanese populations and in alcohol-dependent subjects. Human genetics, 101(2), 243-6. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9402979
Goldman, D., Oroszi, G., & Ducci, F. (2005). The genetics of addictions: uncovering the genes. Nature reviews. Genetics, 6(7), 521-32. doi:10.1038/nrg1635
Heils, A., Teufel, A., Petri, S., Stöber, G., Riederer, P., Bengel, D., & Lesch, K. P. (1996). Allelic variation of human serotonin transporter gene expression. Journal of neurochemistry, 66(6), 2621-2624. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8632190
Hu, X.-Z., Lipsky, R. H., Zhu, G., Akhtar, L. a, Taubman, J., Greenberg, B. D., Xu, K., et al. (2006). Serotonin transporter promoter gain-of-function genotypes are linked to obsessive-compulsive disorder. American journal of human genetics, 78(5), 815-26. doi:10.1086/503850
Lesch, K. P., Meyer, J., Glatz, K., Fliigge, G., Hinney, A., Hebebrand, J., Klauck, S. M., et al. (1997). Neural Transmission Rapid Communication. Journal of Neural Transmission, 1259-1266.
Miller, L. H., & Miller, L. H. (2012). and genetic diseases in Impact of malaria on genetic polymorphism Africans and African Americans.
Mellman, T. a, Alim, T., Brown, D. D., Gorodetsky, E., Buzas, B., Lawson, W. B., Goldman, D., et al. (2009). Serotonin polymorphisms and posttraumatic stress disorder in a trauma exposed African American population. Depression and anxiety, 26(11), 993-7. doi:10.1002/da.20627
Stringer, C.B. (1994). "Evolution of Early Humans". In Steve Jones, Robert Martin & David Pilbeam. The Cambridge Encyclopedia of Human Evolution. Cambridge: Cambridge University Press. p. 242.
Xie, Z., Lee, S. P., Dowd, B. F. O., & George, S. R. (1999). Serotonin 5-HT 1B and 5-HT 1D receptors form homodimers when expressed alone and heterodimers when co-expressed. Pharmacia, 456, 63-67.